HPV Vaccination: A policy imperative or global lobbying at work?
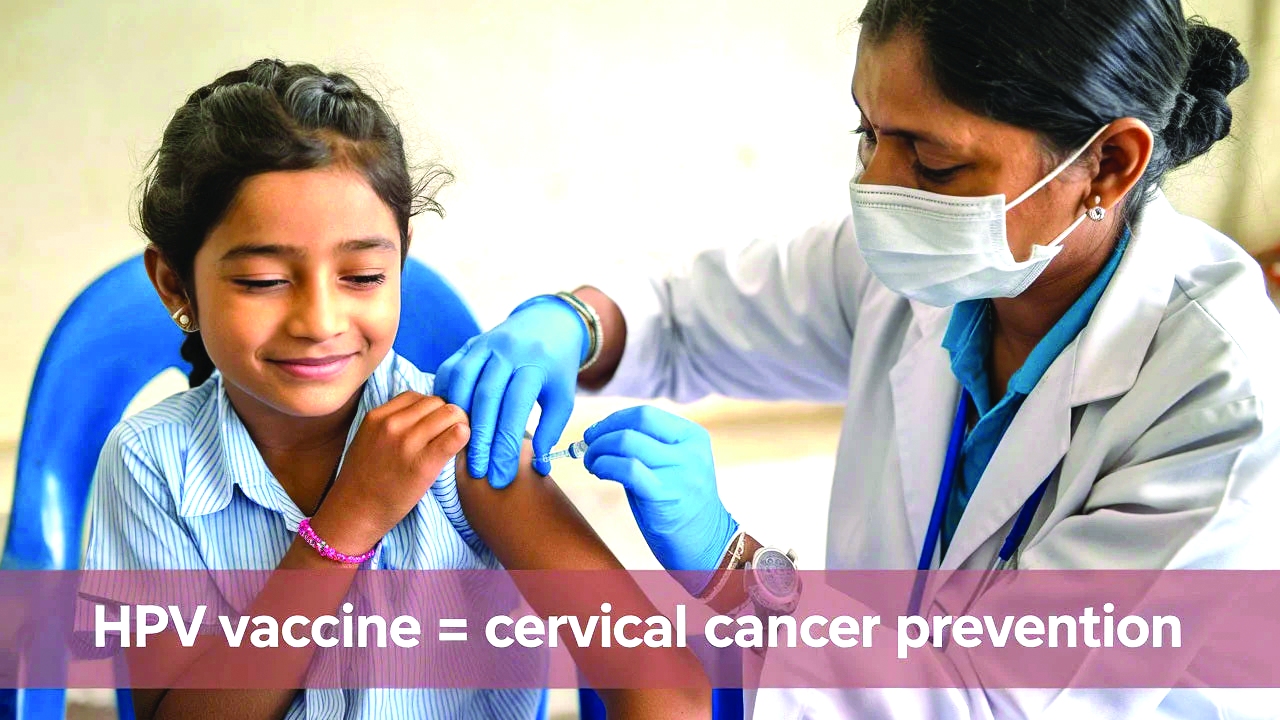
From 28 February 2026, the Government of India launched a single-shot HPV vaccination programme for girls aged 14 years, with a target of 1.15 crore vaccinations each year. The vaccine has been approved by India’s drug regulator, and its supply is being procured through a mechanism in partnership with Gavi, the Vaccine Alliance, which is primarily promoted and funded by the Bill & Melinda Gates Foundation.
This decision has been widely criticised in several quarters for various reasons. Critics argue that it represents a case of interference by a foreign organisation in India’s health policymaking. Secondly, the programme is being promoted with the support of the Gates Foundation, whose activities have long been viewed with suspicion by some observers.
In fact, the Gates Foundation (earlier BMGF) is not being criticised without reason, according to its detractors. In the past, several objections and allegations have been levelled against its co-founder, Bill Gates, regarding controversial experiments allegedly carried out under his direction in different parts of the world. One recent example cited by critics occurred during the India AI Impact Summit 2026, when Bill Gates faced opposition at multiple levels. The controversy stemmed from allegations connected to the so-called “Epstein Files,” which reportedly mentioned extramarital affairs and related issues. As a result, critics say his public image was further damaged and his scheduled programme was ultimately cancelled.
Critics also argue that Bill Gates views India as a laboratory for clinical trials. In 2024, he reportedly stated that India functions as a kind of experimental environment where new initiatives are tested before being expanded elsewhere. The Gates Foundation, however, maintains that his remarks were meant as praise for India’s capacity for innovation and implementation. Nevertheless, based on past experiences with the foundation, critics claim that trials are being conducted in India at his behest, treating Indians as “guinea pigs” for vaccine development.
They argue that such practices would be both unethical and legally questionable.
Trials related to the Human papillomavirus (HPV) vaccine were indeed conducted in parts of India in 2009. At the time, the Parliamentary Standing Committee on Health and Family Welfare criticised the Program for Appropriate Technology in Health (PATH), an organisation associated with the Gates Foundation, for allegedly conducting unethical and illegal trials. According to the committee’s report, several girls reportedly fell ill and some died after being included in HPV vaccine trials without proper informed consent from their parents. The committee recommended strict action against both PATH and the Gates Foundation.
Following protests, the Government of India withdrew the proposal to include the HPV vaccine in the Universal Immunisation Programme in 2018. However, critics claim that intense lobbying by the Gates Foundation later led several state governments to introduce the vaccine in their own vaccination programmes, and that similar efforts continue in other states.
According to these critics, the foundation has been able to influence key policymakers in both central and state governments. They further allege that the foundation attracts former health ministry officials by offering lucrative positions after retirement and maintains influence over some current officials as well.
Supporters of the HPV vaccine argue that cervical cancer primarily results from persistent infection with high-risk strains of HPV, especially types 16 and 18. The risk increases with early sexual activity, multiple sexual partners, weakened immunity (such as in HIV/AIDS), smoking, poor genital hygiene, and multiple pregnancies. Long-term HPV infection can lead to abnormal changes in cervical cells that may eventually develop into cancer if not detected and treated early through screening.
Although the government has presented the vaccination programme as a measure to protect women from cervical cancer, critics point out that the disease-while significant- is the fourth most common cancer globally and the second most common cancer among women in India after breast cancer.
Even so, it currently accounts for only about 10 percent of all female cancers, and its incidence has been declining over time. Another concern raised is the lack of reliable national screening data to accurately determine the number of affected women and their geographical distribution.
Available reports suggest that only a few states-particularly some in North-East India-have relatively higher rates of cervical cancer.
Critics therefore argue that the government should first have launched a comprehensive national screening programme to determine the intensity and regional distribution of the disease before initiating a nationwide vaccination campaign.
Research based on the Global Burden of Disease Study (1990-2019) indicates that the age-standardised incidence rate of cervical cancer in India has been declining, with an average annual reduction of about 0.82 percent between 1990 and 2019. Mortality from cervical cancer declined even faster, at roughly 1.35 percent per year during the same period. This suggests that the overall risk per woman in the population has been gradually decreasing.
Researchers attribute this decline mainly to social changes such as later age at marriage and first childbirth, fewer pregnancies, improved hygiene and living standards, and increased awareness and screening in urban areas. These factors have collectively reduced cervical cancer risk in many parts of India.
By contrast, the incidence of breast cancer has been rising steadily. It has now become the most common cancer among women in India. In 2023, the age-standardised incidence rate of breast cancer was about 29.4 cases per 100,000 women per year, with approximately 2.0-2.03 lakh new cases annually.
The rate has increased significantly-from about 13 per 100,000 women in 1990 to 29.4 per 100,000 in 2023, more than doubling over three decades.
Critics therefore argue that while overall cancer incidence is rising-particularly in the case of breast cancer-the government has not implemented equally strong measures such as large-scale early screening programmes for breast cancer. Instead, they say, it has chosen to prioritise the vaccination of young girls against HPV.
The debate surrounding HPV vaccine advocacy is also complicated by potential conflicts of interest. Some independent researchers have pointed out that a substantial proportion of published research on vaccine safety and efficacy has been funded by, or conducted in collaboration with, pharmaceutical companies.
Given these concerns-along with the earlier controversy surrounding HPV trials, questions about long-term effectiveness in low-screening environments, and the role of pharmaceutical lobbying-critics argue that the Government of India’s decision to launch a nationwide HPV vaccination programme may have been taken too hastily.
They also note that even after vaccination, regular cervical screening remains necessary, and that broader public-health interventions-such as improved sanitation, nutrition, awareness programmes, and affordable screening facilities-may deliver wider health benefits.Finally, critics point out that while India is launching a universal HPV vaccination programme, the uptake of HPV vaccination in the United States has reportedly declined in recent years.
Data from the Centers for Disease Control and Prevention shows that among adolescents eligible for free vaccines through the Vaccines for Children (VFC) programme, the proportion who were up to date on HPV vaccination by age 13 fell by about 10 percentage points for those born in 2010 compared with those born in 2007. Some observers therefore fear that surplus vaccines from other countries may eventually be redirected to markets such as India.
The author is National Co-Convener Swadeshi Jagran Manch Former Professor, PGDAV College, Delhi University; views are personal